Uterine fibroids are non-cancerous growths that develop within or on the uterus, and their classification depends entirely on where in the uterine structure they grow. Submucosal, subserosal, and intramural fibroids each occupy a different layer of the uterus, and that location determines the symptoms a patient experiences, how those symptoms progress, and which treatment approach is most appropriate. Understanding the differences between these three types gives patients the clarity they need to have an informed conversation with their provider about next steps.
What Are Uterine Fibroids and How Are They Classified?
Fibroids, also called uterine leiomyomas, are benign growths made of smooth muscle and fibrous tissue that form within or on the uterus. They are among the most common gynecologic conditions, and while many women have fibroids without experiencing any symptoms, others deal with significant disruption to their menstrual health, pelvic comfort, and fertility. Classification by location is how OBGYN providers organize fibroid diagnosis and treatment planning.
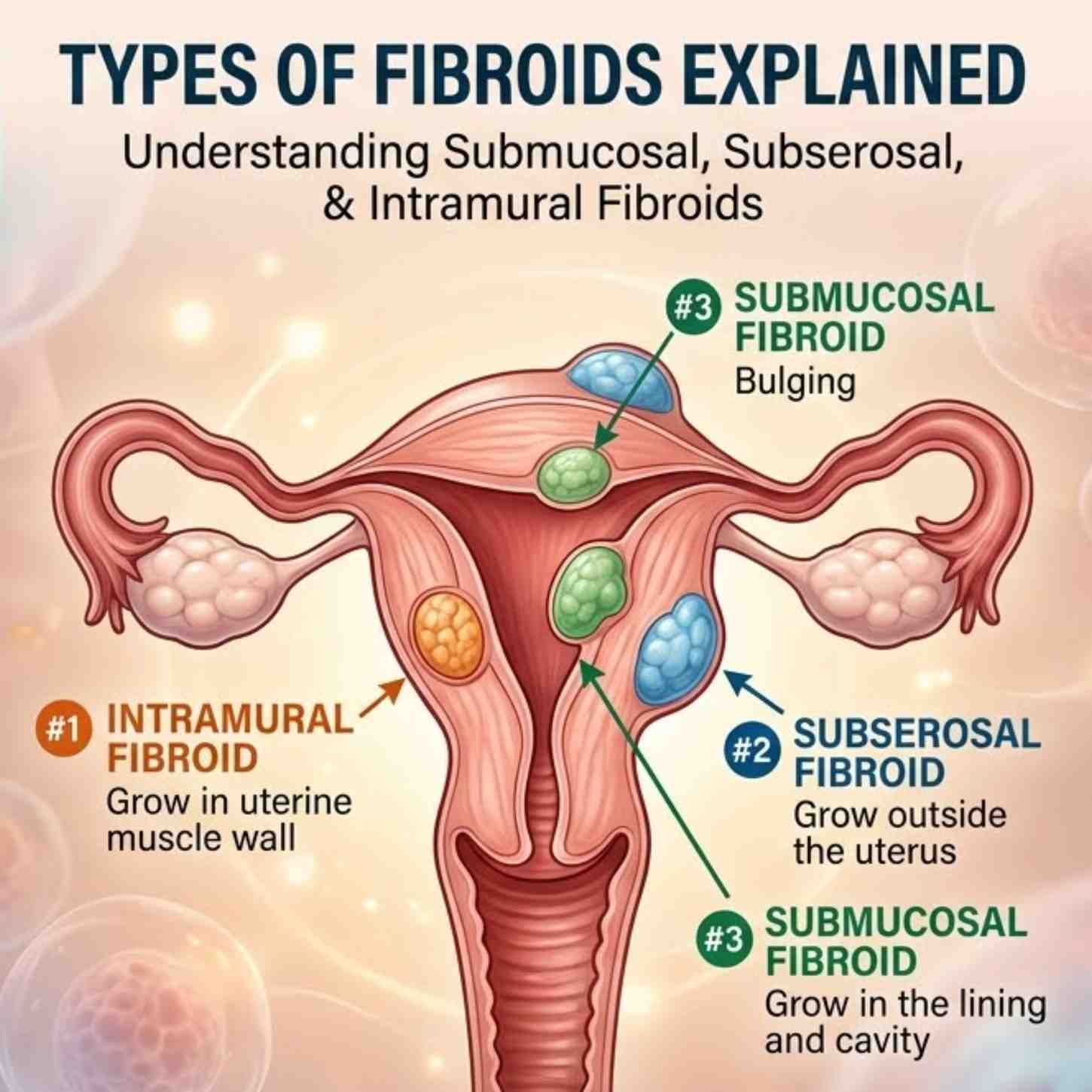
The uterine wall has three distinct layers: the endometrium, which is the inner lining; the myometrium, which is the muscular middle wall; and the serosa, which is the outer surface. Each fibroid type grows in or adjacent to one of these layers. Where a fibroid sits within this structure determines how it interacts with surrounding tissue, which organs it may put pressure on, and how directly it affects menstrual bleeding and reproductive function.
ALSO READ: Fibroids and Fertility: What to Expect
The Three Types of Uterine Fibroids Explained
Each of the three fibroid types has a distinct anatomical location, a recognizable symptom profile, and a different set of clinical implications. Knowing which type is present and how it is positioned is the foundation of any effective treatment plan discussed at an OBGYN clinic. The sections below explain each type in clinical detail.
Submucosal Fibroids
Submucosal fibroids grow just beneath the endometrium, the inner lining of the uterus, and extend into the uterine cavity itself. This positioning makes them the most clinically significant type when it comes to menstrual bleeding and reproductive outcomes. Even a small submucosal fibroid can cause disproportionate symptoms because it sits directly at the interface between the fibroid and the lining that sheds during menstruation.
The symptoms most commonly associated with submucosal fibroids include:
- Heavy or prolonged menstrual bleeding, often severe enough to cause iron-deficiency anemia
- Bleeding between periods
- Pelvic cramping concentrated around the menstrual cycle
- Difficulty conceiving due to the fibroid’s interference with implantation
- Increased risk of miscarriage or recurrent pregnancy loss
For women experiencing unexplained heavy bleeding or fertility challenges, submucosal fibroids are among the first conditions OBGYN specialists investigate. A hysteroscopy, which allows direct visualization of the uterine cavity, is the most precise diagnostic tool for identifying and characterizing submucosal fibroids. Treatment often involves hysteroscopic myomectomy, a minimally invasive procedure that removes the fibroid through the cervix without external incisions.
Subserosal Fibroids
Subserosal fibroids develop on the outer surface of the uterus, growing outward into the pelvic cavity rather than into the uterine cavity. Because they grow away from the endometrial lining, they rarely affect menstrual bleeding directly. Their symptoms are primarily mechanical, driven by the size of the fibroid and the pressure it applies to neighboring structures.
Common symptoms of subserosal fibroids include:
- Pelvic pain, pressure, or a persistent sense of heaviness in the lower abdomen
- Frequent or urgent urination caused by bladder compression
- Constipation or discomfort during bowel movements if the fibroid presses on the bowel
- Lower back pain, particularly when the fibroid grows toward the posterior wall of the uterus
- Abdominal distension or visible bloating in cases of larger fibroids
Subserosal fibroids can grow considerably large before causing noticeable symptoms, which means some patients are unaware they have them until a routine pelvic exam or pelvic ultrasound identifies them. OBGYN care for subserosal fibroids is guided by symptom severity, fibroid size, and growth rate over time. When intervention is needed, laparoscopic or robotic myomectomy are common approaches that allow for fibroid removal with minimal recovery time.
Intramural Fibroids
Intramural fibroids are the most common type overall. They develop within the myometrium, the muscular wall of the uterus, and can grow in multiple directions depending on their position within that wall. When an intramural fibroid grows toward the inner cavity, it begins to behave more like a submucosal fibroid. When it grows toward the outer surface, it begins to produce symptoms more similar to a subserosal fibroid.
Symptoms vary based on size and position but commonly include:
- Heavier or longer menstrual periods when the fibroid distorts the uterine cavity
- Generalized pelvic pressure or a bloated sensation
- Increased urinary frequency if the fibroid puts pressure on the bladder
- Pelvic discomfort that intensifies around menstruation
- Fertility challenges in cases where the fibroid significantly alters the shape of the uterine cavity
Smaller intramural fibroids are frequently discovered incidentally during imaging performed for another reason, and many do not require immediate treatment. Larger ones, or those positioned close to the uterine cavity, warrant closer monitoring and a discussion with an OBGYN about management options. Treatment decisions consider the fibroid’s size, its precise location within the uterine wall, the patient’s symptoms, and reproductive goals.
ALSO READ: Robotic Myomectomy: Benefits of Robot-Assisted Surgery for Health Outcomes
How Fibroid Type Affects Symptoms, Fertility, and Treatment Decisions
Understanding which fibroid type is present shapes every clinical decision that follows, from monitoring frequency to surgical approach. The same symptom, such as pelvic pain, can have very different causes and solutions depending on the type and location of the fibroid producing it. OBGYN specialists use fibroid type as a primary organizing principle when building a treatment plan.
Menstrual and Pelvic Health Implications by Fibroid Type
Submucosal fibroids carry the highest risk of causing significant menstrual disruption. Heavy bleeding from submucosal fibroids can progress to the point where it causes iron-deficiency anemia, with patients experiencing fatigue, shortness of breath, and difficulty maintaining daily function. Intramural fibroids can also contribute to heavier periods when they are large or positioned near the cavity, while subserosal fibroids rarely affect bleeding volume directly but are more likely to cause chronic pelvic pressure and discomfort.
This distinction matters for treatment planning at an OBGYN clinic because the symptom source guides the intervention. A submucosal fibroid driving heavy menstrual bleeding calls for a different surgical approach than a subserosal fibroid causing bladder pressure. Imaging, specifically a pelvic ultrasound or sonohysterogram, is used to classify the fibroid accurately so that treatment addresses the actual anatomical problem rather than symptoms alone.
Fertility Considerations Across Fibroid Types
Fibroid location is a key variable in any gynecological fertility evaluation. Submucosal fibroids are the type most consistently linked to reduced fertility and pregnancy complications. By distorting the uterine cavity, they interfere with implantation and can increase the risk of early pregnancy loss. Intramural fibroids may also reduce fertility, particularly when large enough to alter the shape of the cavity or restrict blood flow to the endometrium. Subserosal fibroids generally have a smaller impact on fertility unless they are exceptionally large or positioned in a way that mechanically affects the fallopian tubes.
For patients pursuing pregnancy, OBGYN care involves evaluating fibroid type alongside other fertility factors before recommending intervention. A myomectomy, which removes fibroids while preserving the uterus, is the standard surgical approach for women who want to maintain reproductive options. The technique used, hysteroscopic for submucosal fibroids or laparoscopic and robotic for intramural and subserosal fibroids, is determined by where the fibroid is located and how it is positioned relative to the uterine cavity.
ALSO READ: Myomectomy vs Hysterectomy: Advantages of Each in Treating Fibroids
Comparing the Three Fibroid Types at a Glance
The table below summarizes the key differences between submucosal, subserosal, and intramural fibroids across location, symptoms, fertility impact, and typical treatment approach.
| Fibroid Type | Location | Primary Symptoms | Fertility Impact | Common Treatment |
| Submucosal | Beneath the endometrium, into the uterine cavity | Heavy bleeding, spotting, cramping | Highest impact on implantation and pregnancy | Hysteroscopic myomectomy |
| Subserosal | Outer surface of the uterus, into the pelvic cavity | Pelvic pressure, bladder and bowel symptoms, back pain | Lower direct impact unless very large | Laparoscopic or robotic myomectomy |
| Intramural | Within the uterine muscle wall | Variable: bleeding and/or pressure depending on size and position | Moderate impact when large or near the cavity | Laparoscopic, robotic, or open myomectomy |
When to Consult a Provider About Fibroids
Many women live with fibroids for years without realizing it. Others notice symptoms but do not connect them to fibroids. If any of the following apply, a consultation with an OBGYN is a reasonable and worthwhile next step:
- Menstrual periods that are heavier than usual or lasting longer than seven days
- Bleeding or spotting between periods
- Pelvic pain, pressure, or bloating that does not resolve between cycles
- Frequent urination that is not explained by a urinary tract infection
- Difficulty conceiving after six to twelve months of trying
- A history of recurrent miscarriage
Fibroids are not a condition to monitor without professional guidance. The earlier a fibroid is identified and classified by type, the more options are available for managing symptoms and protecting long-term reproductive health. Not every fibroid requires treatment, but knowing which type is present and how it is positioned gives both patient and provider the information needed to make a sound decision together.
Roswell Ob/Gyn, LLC provides gynecological evaluations and fibroid treatment including myomectomy across locations in Alpharetta, Atlanta, Canton, and Cumming, Georgia. Schedule an appointment to speak with one of our providers about your symptoms and what your evaluation should include.